The Use of POCUS for Posterior Tibial Nerve Block: A Step in the Right Direction!
Margaret B Rinaldi MD
Aalap Shah MD
Matthew M Moake MD PhD
Ryan M. Barnes DO
Case History
A seven-year-old healthy male presents to the emergency department (ED) with left foot pain after stepping on a needle two days prior. He was seen at an urgent care facility where an X-ray was performed and demonstrated a foreign body in the plantar foot. A point-of-care ultrasound was performed and confirmed the foreign body. Assisted by distraction from child life specialists, a posterior tibial nerve block was performed, and the foreign body was removed under ultrasound guidance. In this case, the patient reported minimal discomfort, even expressing he was unaware that the procedure had occurred after the initial block.
Background
Pediatric puncture wounds are common and are often associated with significant pain.1 The plantar surface of the foot can be difficult to anesthetize, and the posterior tibial nerve block has been shown to provide effective analgesia to this region.2 Multiple studies have shown that the use of ultrasound is associated with improved success of the posterior tibial nerve block.3-5 While there are multiple studies showing the effectiveness of the posterior tibial nerve block, there are few studies that report its usage in the pediatric population.6,7
Anatomy
The posterior tibial nerve provides sensory innervation to the majority of the plantar foot, sparing the most medial and lateral aspects which are innervated by the saphenous and sural nerves, respectively. (Figure 1) The posterior tibial nerve is easiest identified just posterior to the medial malleolus in close proximity to the posterior tibial artery (Figure 1). At this location, both the posterior tibial artery and nerve lie between the flexor hallucis longus and flexor digitorum longus tendons as depicted by ultrasound imaging. (Figure 1)
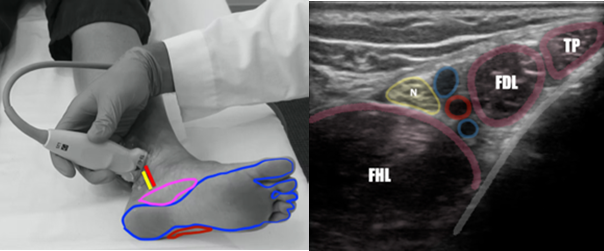 Figure 1. Identification of the Posterior Tibial Nerve in the Distal Ankle. Left: Position of tibial nerve and artery (red/yellow lines) in location of potential blockade and nerve distribution of posterior tibial block (blue), with saphenous nerve distribution (pink) and sural nerve distribution (red). Right: Sonographic anatomy of the PT nerve at the level of the medial malleolus. (FHL=flexor hallucis longus, N=posterior tibial nerve, Red circle= posterior tibial artery, FDL=flexor digitorum longus tendon, TP=tibialis posterior tendon). Image courtesy of Dr. Ryan Barnes
Figure 1. Identification of the Posterior Tibial Nerve in the Distal Ankle. Left: Position of tibial nerve and artery (red/yellow lines) in location of potential blockade and nerve distribution of posterior tibial block (blue), with saphenous nerve distribution (pink) and sural nerve distribution (red). Right: Sonographic anatomy of the PT nerve at the level of the medial malleolus. (FHL=flexor hallucis longus, N=posterior tibial nerve, Red circle= posterior tibial artery, FDL=flexor digitorum longus tendon, TP=tibialis posterior tendon). Image courtesy of Dr. Ryan Barnes
Once the nerve is identified by anatomical landmarks as stated above, it can be tracked proximally to a point where an optimal in-plane needle approach can be obtained, ideally proximal to the Achilles tendon with access to the medial calf. (Figure 2)
 Figure 2. Blockade of the Posterior Tibial Nerve at the level of the mid calf. Left: Ideal in-plane needle insertion proximal to the Achilles tendon. The patient is positioned with clear access to the medial aspect of the ankle and calf. Right: Sonographic appearance at location of block as the needle (yellow line) passes just inferior to the nerve in a path clear of any blood vessels (the blue shaded area indicates where fluid ideally is deposited around the nerve). Image courtesy of Dr. Ryan Barnes
Figure 2. Blockade of the Posterior Tibial Nerve at the level of the mid calf. Left: Ideal in-plane needle insertion proximal to the Achilles tendon. The patient is positioned with clear access to the medial aspect of the ankle and calf. Right: Sonographic appearance at location of block as the needle (yellow line) passes just inferior to the nerve in a path clear of any blood vessels (the blue shaded area indicates where fluid ideally is deposited around the nerve). Image courtesy of Dr. Ryan Barnes
Technique
Position the patient so that there is clear access to the medial malleolus and calf. Notably, the left lateral decubitus position allows for easy positioning with access to the left leg. Use a high-frequency linear transducer. Consideration of needle size should include weighing the need for additional anesthesia at injection site (wheal, LET) versus improvement in needle visualization. A 24-27g needle can be visualized well in superficial tissues, however, for larger patients, larger needle gauges may improve the appearance of the needle (but may also require additional anesthesia at the skin).
First find the posterior tibial nerve and artery just posterior to the medial malleolus. (Figure 1) Then, slide proximally until the Achilles tendon is no longer in view, and the nerve and planned needle path are clear of the vessels. (Figure 2) Using an in-plane needle approach, (Figure 2) guide the needle just inferior to and slightly past the PT nerve. This ensures that any inadvertently injected air does not obscure nerve visualization and allows for a small bit of needle retrograde movement that may occur with hydrostatic pressure from the force of injection. Aspirate to ensure absence of vascular injection, and then deposit 5-7 milliliters of local anesthetic, which should be seen adjacent to, but does not have to surround, the nerve. Of note, do not exceed maximum pediatric or adult anesthetic dosages.
Pitfalls
It is possible to cause injury to local structures: primarily the Achilles tendon and vascular structures. To avoid tendon injury, once the posterior nerve and tibial artery are identified, slide up until the Achilles tendon is outside of view. To avoid arterial injury or inadvertent vascular injection, choose an injection level where the tibial artery either separates away from or sits safely out of the planned needle approach to the nerve.
Integration into Clinical Practice
The posterior tibial nerve block is ideal for patients who sustain plantar surface puncture wound injuries. Using the ultrasound-guided posterior tibial nerve block can be a straightforward and highly effective means of providing analgesia and anesthesia to this area.
References
- Volk A, Zebda M, Abdelgawad AA. Plantar and Pedal Puncture Wounds in Children: A Case Series Study From a Single Level I Trauma Center. Pediatr Emerg Care. 2017;33(11):724-9.
- Colgrove RC. Technique Tip: Posterior Tibial Nerve Block. Foot Ankle Int. 2001;22(10): 839-40.
- Chin KJ, Wong NWY, Macfarlane AJR, Chan VWS. Ultrasound-guided versus anatomic landmark-guided ankle blocks: A 6-year retrospective review. Reg Anesth Pain Med. 2011;36(6):611-8.
- Redborg KE, Antonakakis JG, Beach ML, et al. Ultrasound improves the success rate of a tibial nerve block at the ankle. Reg Anesth Pain Med. 2009;34(3):256-60.
- Shah A, Morris S, Alexander B, et al. Landmark Technique vs Ultrasound-Guided Approach for Posterior Tibial Nerve Block in Cadaver Models. Indian J Orthop. 2020;54(1):38-42.
- Binder ZW, Murphy KM, Constantine E. Ultrasound Guided Posterior Tibial Nerve Block to Facilitate Foreign Body Removal in a School-Aged Child. Glob Pediatr Health. 2020;7:2333794X20947982.
- Moake MM, Presley BC, Barnes RM. Ultrasound-Guided Posterior Tibial Nerve Block for Plantar Foot Foreign Body Removal. Pediatr Emerg Care. 2020;36(5):262-5.